Thoroughly documenting these communications creates a comprehensive, compliant record that supports continuity of care and legal accountability. Accurately documenting communication helps PIC meet HIPAA’s requirement to maintain comprehensive records of patient-related communication. Documentation about communication also supports continuity of care, ensuring all members of the PIC care team have access to a complete patient history.
The RainTree communication tab of the child's chart documents the disclosure log (sending or receiving faxes), calls and texts made for service coordination with or for the family, requesting information, and to indicate the final step of exiting a child, 45-day pends and exit prior to prior to enrollment. Other communication that is not in a daily note will be logged here. Keep in mind that logs can be subpoenaed and while not typically released to the family, may be released.
To find the communication tab select the client from the patient list and select Chart
The Communication Tab is the fourth tab:
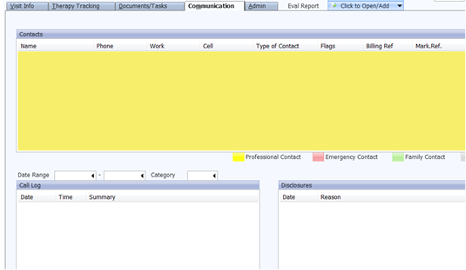
You will see three boxes:
Contacts Box-This is where a list of people involved with the care of the child are listed. Contacts can be added by selecting ADD and completing the information .The Drop Down box under “Contact Type” has a list of the most common relationships. This list can be expanded if there are others we use consistently.
Call Log-Is the location where we would document telephone calls or other communications regarding a child’s care or services.
To better identify the nature of the call, use the category “Freeform Description” box. Pick from the drop down menu.
When to add to the communication log
All communication log notes should include the following accurate information:
- Date/time of communication
- Name(s) of individuals involved
- Summary of information discussed
All communication log notes need to be signed off to be included as part of the electronic medical record. Keep in mind that logs can be subpoenaed and while not typically released to the family or legal system, they may be released.
- Communication with the family members/caregivers via phone call, texts, and/or email (if sent outside of RT) regarding:
- appointment reminders
- follow-ups
- instruction
- updates from the family,
- ANY communication involving PHI*.
*PHI includes the patient’s name, dates related to patient's health or identity, phone number, email address, information regarding treatment or conditions, etc. This includes all methods
- Consultation with other health professionals once a Release of Information has been signed by the guardian.
Examples include (but are not limited to):
- Calling or texting the family to schedule, discuss updates, review insurance information, or follow up on signature forms.
- Phone conversations with outside therapy clinics for coordination of care
- Updates from the family between visits.
- Coordination with OCS
- Referral information
Automated task categories- these will start an automatic process once the comm log note is signed off:
- 45Days Family Pend: Pend requests, under category
- Change in Placement: when a child's address or placement has changed
- Exit/LTFU/Decline/WNL: Exit reason prior to enrollment under category
- Screen to Evaluation: If a child has had a developmental screening and the provider recommendation is for a full evaluation