Part C Eligibility Categories and Definitions
Part C Eligibility: The DHSS EI/ILP assures that children, birth to three years shall be eligible for early intervention services under Part C of IDEA, if the multidisciplinary team finds any one or more of the following exist, the ILP will enroll the child for services: developmental delay, physical or medical condition as determined by the state, or observed significant atypical development (determined using Informed Clinical Opinion).
A. Developmental Delay—A child experiencing a 50% delay based on age equivalent skills or equivalent standard deviations below the norm in one or more of the following areas: cognitive; physical (including vision and hearing, fine and gross motor skills); communication (language, speech and communication); social and emotional development and adaptive development.
(34CFR, 303.21 (a) (1)
B. Physical or Medical Condition: An infant or toddler may be eligible for Part C when she/he has a diagnosed physical or medical condition that has a high probability of resulting in a developmental delay including, but not limited to the listed in 34CFR 303.21 (a)(2)(ii)
C. Informed Clinical Opinion: (taken from Part C Credential)
Informed clinical opinion is used by professionals in the evaluation process to make a recommendation as to the initial and continuing eligibility. Informed clinical opinion 34CFR 303.321 (a)(3)(ii) may be used by an evaluation team to determine eligibility when the approved tool(s) or other domain-specific tool(s) are not able to establish a developmental level due to the age of the infant or the child’s level of arousal and ability to participate at the time of the evaluation ; or when there are inconsistencies in the child’s performance or inconsistencies in the results of the evaluation and the team determined that the child has significant atypical development.
- Informed clinical opinion means the knowledgeable perceptions of the evaluation team who use qualitative and quantitative information regarding aspects of a child’s development that are difficult to measure in order to make a decision about the child’s eligibility.
- Informed clinical opinion in accordance with these policies may be used if a clear developmental level cannot be gained through the use of approved tool(s) or domain-specific tools; or when there are inconsistencies in the child’s performance or inconsistencies in the results of the evaluation; and shall be documented as “significant atypical-development”.
- In no event may informed clinical opinion be used to negate the results of evaluation instruments used to establish Part C eligibility.
A. Developmental Delay:
The child’s developmental delay must be:
- Measured and verified by appropriate approved diagnostic instruments and procedures that determines percent delay.
- On the primary evaluation, the primary service provider will complete this section
B. Physical or Medical Conditions (34CFR 303.21 (a)(2)(ii)): (updated from ILP Operations Manual 05/07/2026)
- Adjustment Disorder
- AIDS or HIV Positive
- Anxiety Disorder of Infancy and Early Childhood
- Arthritis
- Autism Spectrum Disorder
- Blind or Visually Impaired, Significant/Progressive
- Central Nervous System deficit or degenerative disorder
- Cerebral Palsy
- Chronic Lung Disease
- Chronic Otitis Media longer than 6 months
- Cleft Palate with or without Cleft Lip
- Complex Seizure Disorder
- Cornelia de Lange syndrome
- Cystic Fibrosis
- Cytomegalovirus (CMV), congenital
- Deaf or Hard of Hearing, Significant/Progressive
- Deafblind
- Disorders of Affect
- Disorders of Relating or Communicating
- Down Syndrome
- Dwarfism
- Epilepsy
- Failure to Thrive
- Fetal Alcohol Spectrum Disorder
- Fragile X Syndrome
- Hearing Impairment, Significant/Progressive
- Heart Disease, Congenital
- Hydrocephaly
- Microcephaly
- Muscular Dystrophy
- Myelomeningocele
- Neurological impairment
- Orthopedic Impairment
- Other (Diagnosis typically associated with substantial developmental delay)
- Periventricular Leukomalacia, unresolved
- Posttraumatic Stress Disorder
- Prader-Willi Syndrome
- Reactive Attachment Disorder
- Renal agenesis with or without hypospadias
- Rubella, congenital
- Spina Bifida
- Toxoplasmosis, congenital
- Trisomy 13
- Trisomy 18
- Turner Syndrome
Uncontrolled maternal PKU
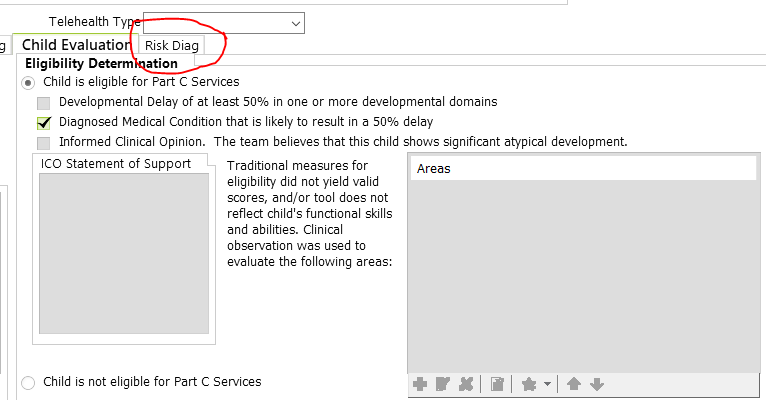
On the primary evaluation, the primary service provider will complete this section, and is required to complete and additional 'Risk Diag' tab circled below in red ( will allow you to indicate medical diagnosis):
Child qualifies by Medical Diagnosis, but is functioning Within Normal Limits: the family and child must still be offered the opportunity to enroll or to decline services. In these cases, since no therapeutic interventions are indicated, the family is offered Family Service Coordination (FSC). The family may also be offered periodic developmental screenings, evaluations, referrals or connections to other needed community services. This situation is uncommon. See FSC only IFSP.
C. Informed Clinical Opinion:
ICO is an eligibility category to enroll children who experience significant atypical development in one or more areas, that is not captured by evaluation and may or may not be measurable with other assessment tools, but minimally is observed by provider and reported by family or record.
This is not for children who are at risk of developmental delays due to circumstances—but for children who experience delays that are difficult to measure. Do not use RISK to justify ICO. Focus on evidence of delay.
On the primary evaluation, the primary service provider will complete this section. Ask for support from the co-evaluator if eligibility falls into an area you did not evaluate:
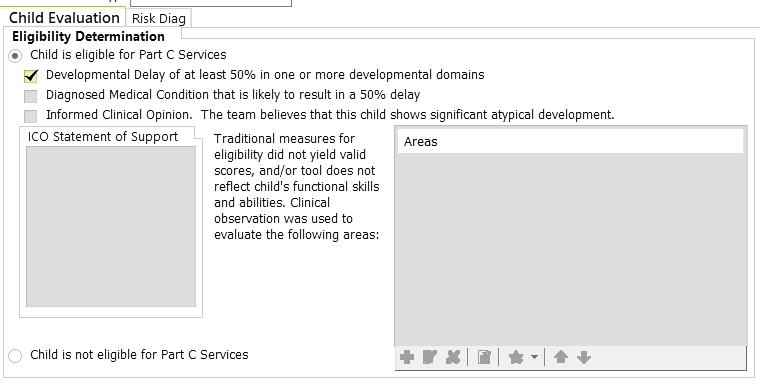
Select the “Child is eligible for Part C services” and the ICO box, if they do not qualify by 50% or medical condition, and demonstrate significant atypical development.
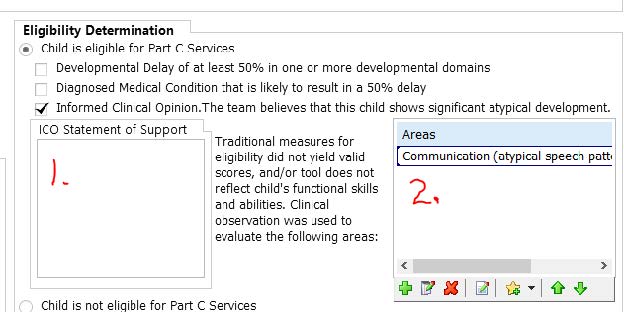
For area #1, depending on how the child presents, providers will choose a statement of support, and can edit the following as needed:
For a significant delay (RainTree Global Abbreviation-- icoalmst50): IDA-2 demonstrates substantial but not qualifying delay (ie, 45% delay in two areas):
- Statement: The IDA-2 results show this child experiences substantial delay(s). The considerable, qualitative delays that were observed include [enter observed delays examples from handout]. While the child does not qualify for Part C by evaluation scores, the child does qualify by ICO because these delays significantly interfere with the child's functioning in daily routines and activities and across environments.
Delay not captured (RainTree Global Abbreviation-- iconotcapt): Child demonstrates a concerning difference (delay) that is not captured on the IDA-2 (may be captured on other tools such as the REEL, and is observed, or observed only):
- Statement: This child demonstrates significant, qualitative delays including [enter observed delays examples from handout] and [if other test scores: name them here]. The observed delays substantially interfere with the child's functioning in daily routines and activities and across environments. The IDA-2 results do not demonstrate the child’s observed delay, so the child does not qualify for Part C by evaluation scores, but does qualify as a result of observed delays.
After Annual evaluation (RainTree Global Abbreviation-- icoannual): the child continues to show a delay (substantial or not captured by IDA-2) but not 50% delay:
- Statement: While the child has made gains during enrollment in Part C services, the child continues to demonstrate significant, qualitative delays including [enter observed delays from handout] and [if other test scores: name them here]. These delays substantially interfere with the child's functioning in daily routines across environments. Since the IDA-2 results do not demonstrate the observed delay, the child qualifies for Part C based on the above cliniical concerns.
For area #2, providers click the predominant area(s) affected.
List of Statements of Observed Delay for ICO
During the intake or evaluation, a provider has observed that the child has skills that are not generalized, or, may demonstrate splintered skills in one or more developmental areas, and while difficult to measure can support qualifying a child for Part C by ICO.
Gross Motor
- Lacks general strength/muscle tone of all parts of body
- Posture concerns, alignment of joints
- Struggles with balance, static and dynamic
- Limited flexibility (muscles)
- Limited range of motion (joints)
- Does not like to move or fearful
- Frequency/amount is insufficient or much more than expected
- Substantial amount of support/assistance needed
- Compromised or very limited movement (quality)
- Needs equipment/devices to move through environments
- Limited or compromised rotation (ie, more linear movement patterns)
- Not progressing with “Mini milestones” (e.g. transitional positions between motor milestones)
- Limited endurance
- Limited awareness of safety – stairs/playground/equipment
Fine Motor
- Using a motor skill pattern that is immature (whole hand grasp, no pincer yet, etc)
- Limited or not engaged in utensil grasp
- Does not isolate index finger for poking/pointing
- Has had very limited opportunity/exposure (parent report)
- Heavy handedness/quality, or limited or absence of graded movement
- Visual motor – child does not maintain visual attention to grasp/release/play
- Not using both hands in coordination as expected for age, Limited bimanual skills (e.g. stabilizing toys with one hand while acting on with other)
Relationship to objects
- Demonstrates repetitive play
- Limited imaginative play
- Engaged in lining up toys
- Not vocalizing in play “talking to toys”
- Limited or not functional play vs not playing appropriately
- Hyper focused (close examination only of objects)
- Too much movement from toys to toys or place to place, wandering play, climbing
- Limited or not engaged in meaningful play
- Not inviting others to join play (ie, during kitchen pretend play, or referencing toys/interactions)
- Limited interactions with others (parallel vs interactive play, close exam only of objects)
Communication
- Very quiet/not engaged or never engaged in babble
- Limited or rigid communication patterns
- Not using or limited gestures (in addition to pointing)
- Not using or limited signs
- No or limited progress gaining vocabulary
- Do not attend to items pointed out by others
- Extremely difficult to understand by caregivers and others
- Limited use of words to label/request
- Limited response to labels/requests from others
- Consistently demonstrated a very limited understanding of others
- Does not make eye contact consistently
- Needs consistent support from caregivers to interact with others, needs additional cues to follow directions, get needs met
Self-help/Sensory
- Limited number of favorite activities in day
- Unable to or limited ability to engage in bath time
- Unable to successfully engage in transitions – quality of
- Unable to or limited ability to ride in car
- Strong reaction to sensory play/experience (messy, sticky, textures)
- Unable to feed self/disrupted or difficult feeding
- Does not tolerate clothes
- Vision/hearing sensitivities
- Sleep schedule is consistently disrupted, cannot fall asleep on own, struggles accepting support, wakes hourly, several hours needed to fall asleep
Relationships
- Hits, kicks, bites caregivers or other children
- Does not or limited ability to seek comfort and withdraws
- Does not interact with others
- Does not make eye contact, or very limited
- Limited or no engagement with caregiver as safe harbor or secure base
- Other delays significantly impede child’s relationships
- Does not access parent using safe harbor or secure base behaviors
Coping/Social Emotional/Feelings
(consider absence, duration, frequency and intensity)
- Intense upset behaviors
- Does not or limited ability to engage with others
- Unable to play alone, consistently clinging across environments and caregivers
- Child consistently does not discriminate between caregivers, siblings or others
- Does not respond to or limited ability to calm
- Consistent limited participation or withdrawal from caregivers or others
- Consistent behaviors that interfere with engaging in environments
- Tantrum, physicality to cope
- Hyper focus
- Child not able to play with other children their age if age-appropriate
- Child is not responsive to or tuned to behaviors/emotions of others
OCS involvement
(consider what impedes development or functioning)
- Dysregulation (significant disruption in functioning, difficult behaviors, delay in some skills, loss of skills) as a result of changes in environment/relationships (new relationships, loss of stabilizing relationships
Low Incidence Disorders: Hearing and Vision, State of Alaska Guidelines
Hearing Loss
If you have a child that has documented hearing loss in the file:
- Obtain medical records including an audiogram from an audiologist, and check to see if it meets the Part C Medical Diagnosis specifications.
- If they do not qualify with a Medical Diagnosis, check for delays at 50% or greater in combination with the documented hearing loss for Part C Developmental Delay.
- If they do not meet Medical Diagnosis or Developmental Delay, check for any delay or atypical factor related to hearing loss as determined by the team for a Part C Informed Clinical Opinion.
- If the child does not meet specifications for any category, they are NOT Eligible. (If the team agrees, suggest a follow up evaluation or check-in for 6 months later as many delays and atypical factors present or become more significant later for children with hearing loss.) Family may always re-refer at any time otherwise.
| Age | Hearing Eligibility Criteria | Documentation |
|---|---|---|
| 0-3 Years Old | Eligibility criteria for Part C Medical Diagnosis services for infants and toddlers with hearing loss
| Documented hearing loss a 40dB+ in two or more frequencies, bilaterally (pure tone), diagnosed by an audiologist. (Also, check for specific syndromes if the Hearing Loss is the result of a syndrome.) |
Eligibility criteria for Part C Developmental Delay services for infants and toddlers with hearing loss
| A child with any type, degree, or configuration of hearing loss as documented by an audiologist (NOT Part C Medical Diagnosis eligible) and has a 50% delay in one or more developmental domains. | |
Eligibility criteria for Part C Informed Clinical Opinion services for infants and toddlers with hearing loss
| A child with any type, degree, or configuration of hearing loss as documented by an audiologist (NOT Part C Medical Diagnosis eligible), some delays in the domains (NOT Part C Developmental delay eligible) or significant atypical development with one or more factors related to hearing loss (listed below) that is difficult to measure, and is determined by a team. Factors include but are not limited to:
| |
| 3-21 Years Old | Eligibility criteria for Part B services for preschool children with hearing loss | Deafness or hearing impairment that adversely affects educational performance and requires special facilities, equipment or methods to make his/her educational program effective and be diagnosed by a physician or audiologist and be certified as qualifying for and needing such services. |
Blind or Visually Impaired, Significant/Progressive
If you have a child that has documented vision loss in the file:
- Obtain medical records including information from an opthalmologist, and check to see if it meets the Part C Medical Diagnosis specifications.
- If they do not qualify with a Medical Diagnosis, check for delays at 50% or greater in combination with the documented vision loss for Part C Developmental Delay.
- If they do not meet Medical Diagnosis or Developmental Delay, check for any delay or atypical factor related to vision loss as determined by the team for a Part C Informed Clinical Opinion.
- If the child does not meet specifications for any category, they are NOT Eligible. (If the team agrees, suggest a follow up evaluation or check-in for 6 months later as many delays and atypical factors present or become more significant later for children with vision loss.) Family may always re-refer at any time otherwise.
| Age | Vision Eligibility Criteria | Documentation |
|---|---|---|
| 0-3 Years Old | Eligibility criteria for Part C Medical Diagnosis services for infants and toddlers with vision loss
| The following diagnoses indicate “Significant/Progressive Vision Impairment” for Part C eligibility:
|
Eligibility criteria for Part C Developmental Delay services for infants and toddlers with vision loss
| A child with any type, degree, or configuration of hearing loss as documented by an audiologist (NOT Part C Medical Diagnosis eligible) and has a 50% delay in one or more developmental domains. This is determined by the use of a standardized test. | |
Eligibility criteria for Part C Informed Clinical Opinion services for infants and toddlers with hearing loss
| There can be a qualification of “Significant/Progressive Vision Impairment” by Clinical Opinion when there is a high risk for a vision impairment diagnosis due to medical history (prematurity, birth injury, IVH, diagnosed syndrome, etc.) and visual skills less than expected for developmental age as assessed by a vision impairment educational specialist. The following diagnoses may qualify as “Significant/ Progressive Vision Impairment” by Clinical Opinion and should be considered for Part C eligibility with additional evaluation and information:
| |
| 3-21 Years Old | Eligibility criteria for Part B services for preschool children with hearing loss | Vision loss that adversely affects educational performance and requires special facilities, equipment or methods to make the child’s educational program effective and be diagnosed by a physician or audiologist and be certified as qualifying for and needing such services. |